
Clinical Treatment of C. auris Infections —
Key Points
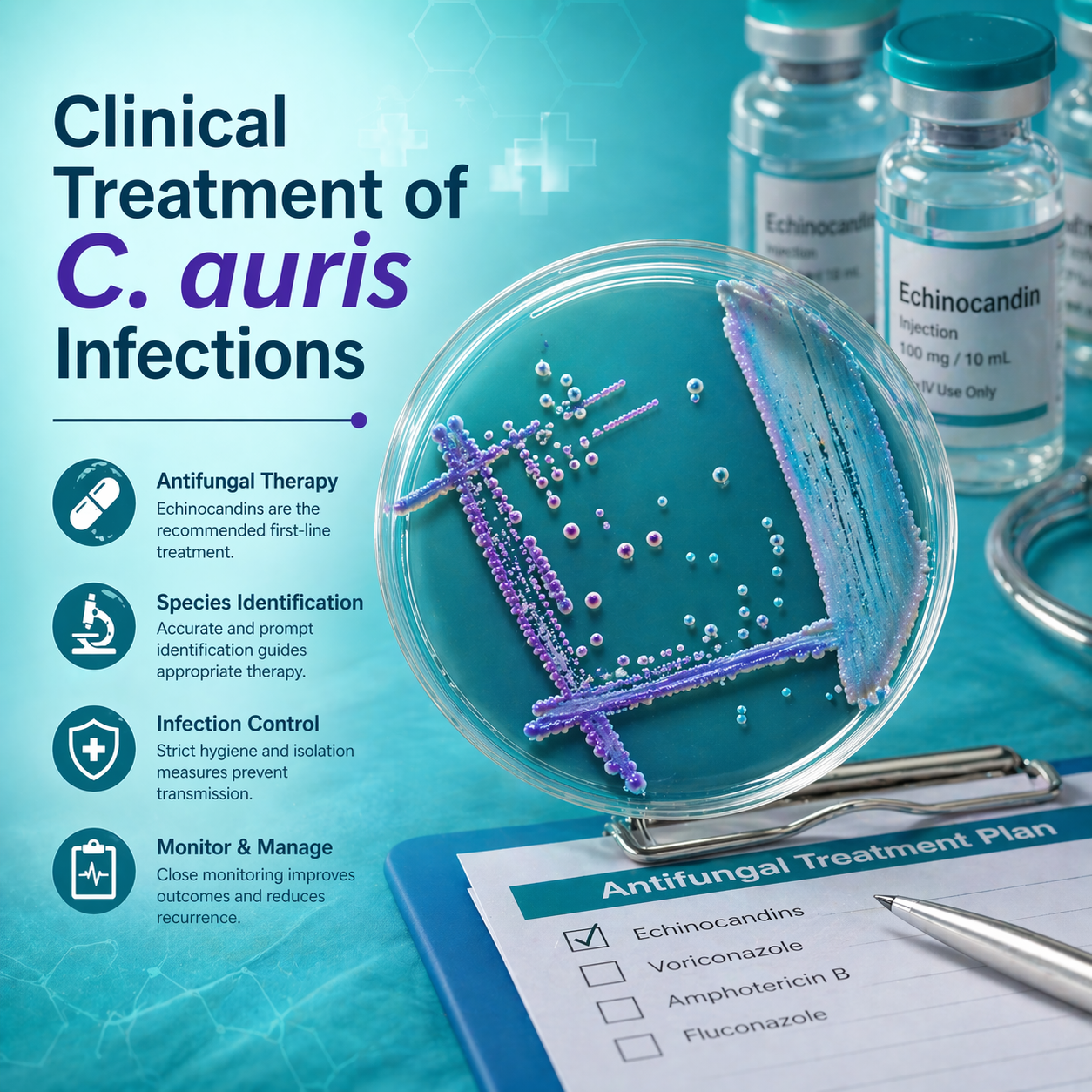
Candida auris (C. auris) infections require antifungal therapy only in clinical disease, not in colonization or screening-positive asymptomatic patients.
Core Treatment Principles
- Treat only clinical infections (no treatment for colonization or noninvasive detection).
- Echinocandins are the first-line therapy for adults and children > 2 months.
- Amphotericin B deoxycholate (1 mg/kg daily) is first-line for infants < 2 months.
- Increasing reports of echinocandin resistance and pan-resistance.
- Investigational antifungals may be considered for resistant cases.
- All confirmed cases should be reported to public health authorities.
- Strongly consider infectious disease specialist consultation.
- Adjust therapy based on patient factors, response, and susceptibility testing.
Critical Treatment Restriction
- No antifungal treatment is recommended for:
- Colonization cases
- Positive screening without symptoms
- Detection in noninvasive sites (e.g., urine, respiratory tract)
Adults & Children ≥ 2 Months — First-Line Therapy
Echinocandin-based regimens:
- Anidulafungin
- 200 mg IV loading dose → 100 mg IV daily
- Not approved for pediatric use
- Caspofungin
- 70 mg IV loading dose → 50 mg IV daily
- Pediatrics: 70 mg/m² loading → 50 mg/m² daily (BSA-based)
- Micafungin
- 100 mg IV daily
- Pediatrics: 2 mg/kg/day IV
- May increase to 4 mg/kg/day in children ≥ 40 kg
Neonates (< 2 Months)
- First-line:
- Amphotericin B deoxycholate: 1 mg/kg daily
- If no response:
- Liposomal amphotericin B: 5 mg/kg daily
- In rare cases (CNS disease excluded):
- Caspofungin: 25 mg/m²/day IV
- Micafungin: 10 mg/kg/day IV
Antimicrobial Resistance Considerations
- Rising cases of:
- Echinocandin-resistant strains
- Pan-resistant strains (resistant to all major antifungal classes)
- If echinocandin resistance suspected or confirmed:
- Switch to liposomal amphotericin B (5 mg/kg daily)
- If no clinical improvement after ~5 days of echinocandin therapy:
- Reassess for resistance and consider alternative therapy
- If pan-resistant infection:
- Consider investigational antifungal agents
Long-Term Infection Control
- Patients often remain colonized long-term or indefinitely even after successful treatment.
- Continuous adherence to infection prevention and control measures is required throughout and after therapy.
Monitoring & Reporting
- Closely monitor:
- Clinical response
- Drug toxicity
- Susceptibility testing results
- Report all cases to:
- Local or state health departments